Lung cancer
Lung cancer accounts for nearly one-fifth (18%) of all deaths due to cancer. Prevention measures combined with appropriate early detection, treatment, and care can help reduce this significant burden of disease.

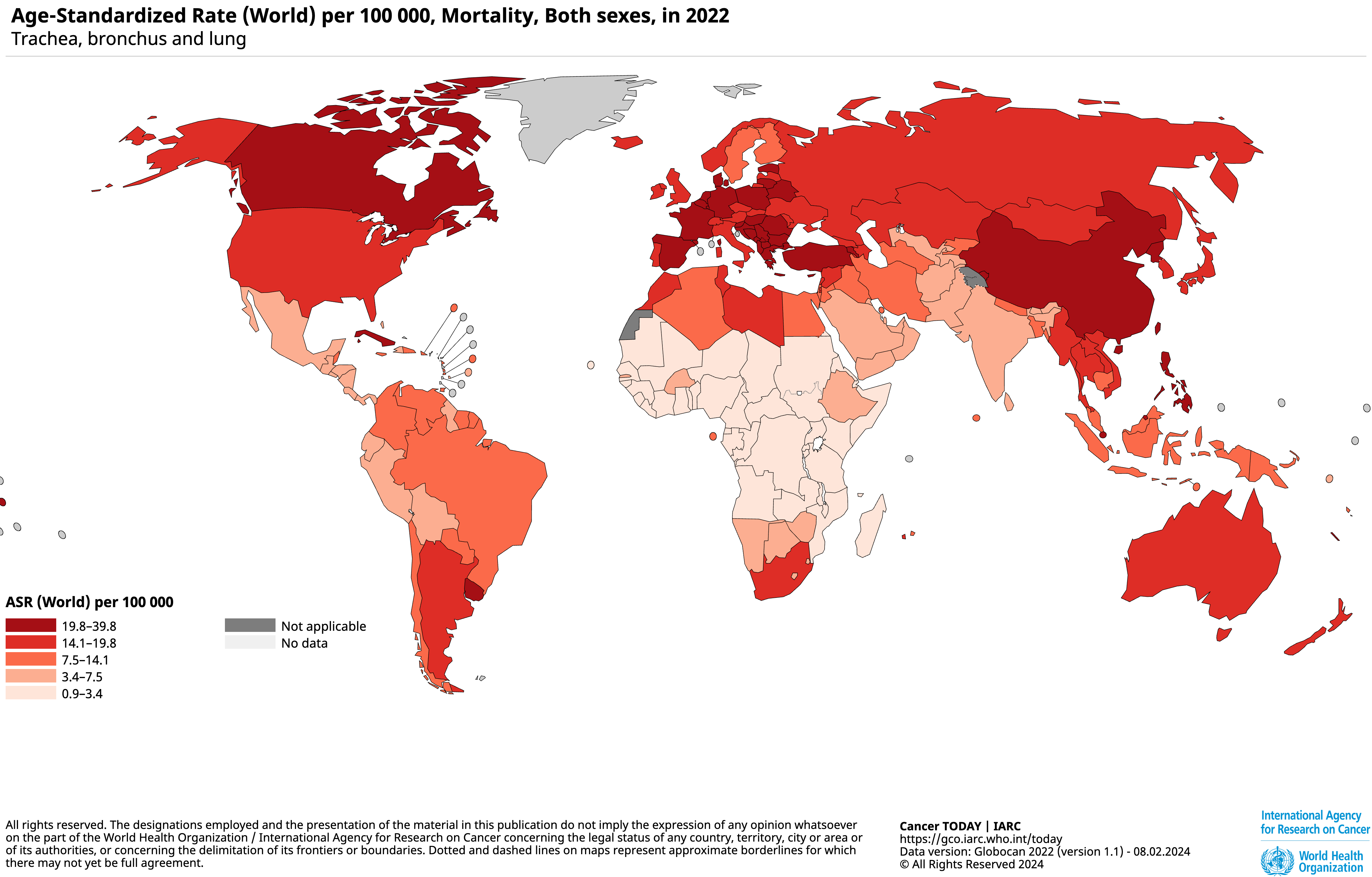
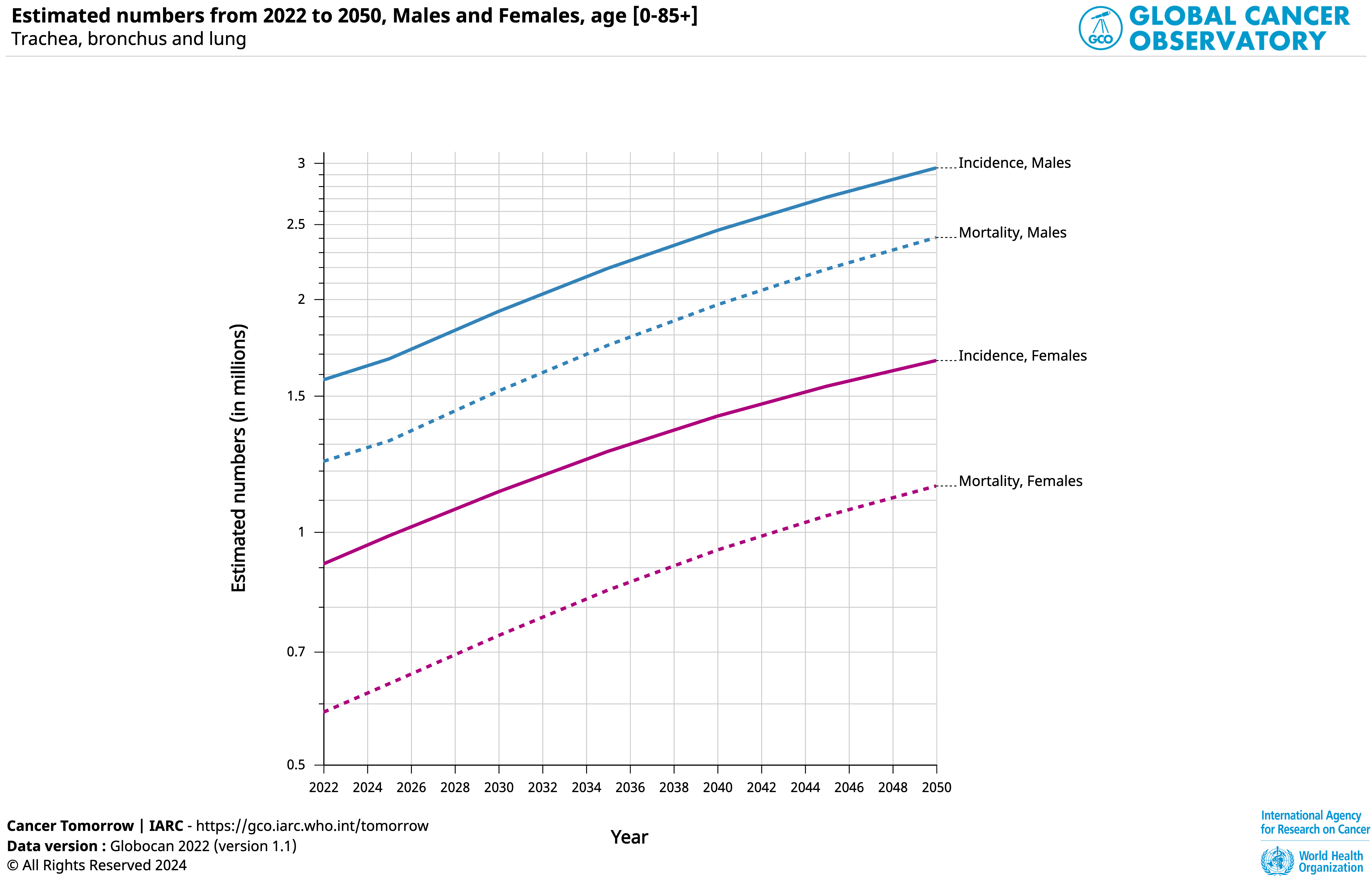
Lung cancer is the most diagnosed cancer globally (both for men and women), with nearly 2.5 million new cases every year. It is also the leading cause of death due to cancer (Globocan 2022), claiming 1.8 million lives annually. Without global efforts, lung cancer deaths are projected to rise by 30% by 2035.[1]
Tobacco consumption, second-hand smoke, outdoor and indoor air pollution, exposure to asbestos and radon are the main preventable causes of lung cancer. Tobacco smoking is the leading risk factor for lung cancer,[2] with non-smokers exposed to second-hand smoke have a 20-30% higher risk of developing lung cancer.[3]
In terms of mortality, estimates suggest that tobacco consumption is responsible for over 67% of lung cancer deaths worldwide, air pollution for 29% of lung cancer deaths, and asbestos exposure about 10% of lung cancer deaths, with significant overlap between these categories. Critically, each of these risk factors can be reduced by evidence-based policies.
Lung cancer is the leading cause of cancer death globally, driven by tobacco use, air pollution and inequities in exposure, but prevention and early detection can save lives.
While lung cancer incidence and mortality rates are highest in high-income countries (HICs), these regions are experiencing declines in the number of new lung cancer cases and related mortality due to decreases in tobacco use and advancements in and access to new treatments. Declines in tobacco consumption can be attributed to effective control measures, such as those outlined by WHO’s Framework Convention for Tobacco Control,[5] a reduced exposure to asbestos, and improved air quality.
In contrast, low- and middle-income countries (LMICs) are in the later phases of the tobacco epidemic, where they are still experiencing high rates of tobacco-related illnesses and deaths due to prolonged use and less established control measures including rising lung cancer incidence and mortality. Cities in low-resource settings also suffer from high rates of air pollution.[6]
The implementation of prevention policies is a key factor in reducing the risk of developing lung cancer, while early diagnosis at the onset of disease significantly improves five-year survival rates, from less than 10% at stage four to 63-65% at stage one.[3][4] It also reduces healthcare costs by two to four times compared to late-stage treatment.
Although low-dose CT screening can lower lung cancer mortality,[5] the adoption of lung cancer screening programmes has been slow,[6] with uptake remaining limited compared to other cancer screening initiatives.
The World Health Organization (WHO) recommends combining public awareness, health services, and equipped health workers for timely diagnostics, especially given the absence of symptoms in many stage-one lung cancer cases. [7]
Click on images below to view them larger
Providing lung health for remote communities
Helping radiologists identify lung cancer
The lung cancer care pathway [12]
Optimal Care Pathways, developed in Australia as part of a national initiative to improve cancer care outline best practices in cancer service delivery, from prevention and early detection to diagnosis, treatment, recovery, and end-of-life care. These pathways serve as a comprehensive guide to ensure consistent, high-quality, and evidence-based care for cancer patients.
The pathways are built on multiple key principles:
- Patient-centred care – Prioritising individual needs and preferences.
- Safe and quality care – Ensuring treatment meets the highest safety and quality standards.
- Multidisciplinary care – Bringing together expertise from multiple specialties.
- Supportive care – Offering comprehensive support services to patients and families.
- Care coordination – Streamlining care across providers and services.
- Communication – Promoting clear and compassionate dialogue with patients and their care teams.
- Research and clinical trials – Encouraging access to the latest evidence-based treatments and trials.
These principles guide health professionals and services in providing optimal treatment, enhancing patient outcomes, and supporting people living with cancer and their families every step of the way. It is important to note that not all patients will follow every step of the pathway.
Applied to lung cancer, the components of the care pathway can include:
- Prevention and early detection, addressing smoking cessation, exposure to second-hand smoke, indoor and outdoor air pollution, asbestos and radon, as well as risk factors assessment, personal and family history completed by screening recommendations.
- Primary health care and referral, including sign and symptoms awareness, primary healthcare workforce training, referral options and time to diagnosis.
- Diagnosis and treatment referring to screening modalities such as spirometry, PET-CT and CT scans, molecular testing, innovative tools development and tumour board meetings. Discussions about appropriate treatment planning such as radiation therapy, surgery, and other options according to staging.
- Survivorship, supportive care and end-of-life care ensuring access to detection of recurrent disease, referral and recall systems. Developing advance care programmes including referral to palliative care considering the care environment
UICC’s actions to advance global lung cancer care
UICC is dedicated to elevating global efforts to improve lung cancer prevention, early detection, treatment, and survivorship. It does so through strategic engagement and collaboration with a diverse network of stakeholders.
UICC’s work brings together a variety of essential partners, including civil society organisations (CSOs), the private sector, policymakers, health professionals, foundations, and patient advocacy groups.
UICC works closely with Permanent Missions in Geneva and governments to support lung cancer initiatives, facilitating global alignment and reinforcing national efforts. Recognising the need for more urgent action on lung health, UICC is working with partners on a lung cancer resolution to present at the upcoming World Health Assembly in May 2025.
Supporting Development and Knowledge Sharing
-
Technical Resources: UICC collaborates with key global health bodies, such as the International Agency for Research on Cancer (IARC) and WHO, to create and distribute technical resources that strengthen lung cancer programmes worldwide.
-
Global cancer control agenda: UICC’s objective is to integrate lung cancer comprehensively into the global cancer control agenda, ensuring it receives the attention it deserves on a global scale.
-
Knowledge and information sharing: Through ongoing dialogue and shared insights, UICC empowers key stakeholders with the knowledge needed to improve lung cancer outcomes.
Together, UICC aims to transform the landscape of lung cancer care worldwide, making progress for a healthier future for all.
The Lung Cancer Collaboration
The Lung Ambition Alliance (LAA) and the World Economic Forum (WEF) launched a partnership at the WEF’s Sustainable Development Impact Summit in 2021 called the Lung Cancer Collaboration. This multi-stakeholder crosssectoral collaboration aims to double five-year survival in lung cancer by 2030, in line with the broader goal of reducing premature deaths from non-communicable diseases by one-third by 2030, the focus of the United Nations’ (UN) Sustainable Development Goal (SDG) 3.4.
Since October 2021, three working groups were formed to develop key actions and recommendations for the collaboration. In May 2022, the LCC published a report including recommendations on early detection and screening, financing and quality of care.
Since 2023, the LCC secretariat has been hosted and led by UICC with a long-term ambition to drive commitment for urgent, coordinated global action on improving lung cancer survival by recommending and supporting the implementation of targeted efforts on lung cancer care.
The collaboration aligns with and complements the work of other lung cancer initiatives such as the Global Lung Cancer Coalition and the Lung Cancer Policy Network.

The Lung Cancer room is a dedicated space for the lung cancer community to stay connected, share knowledge, and exchange key insights from lung cancer experts.
What is lung cancer?
Lung cancer is a type of cancer that begins in the lungs. It is the leading cause of cancer deaths worldwide. Lung cancer can occur in people who smoke, as well as in those who have never smoked.
The main types of lung cancer are non-small cell lung cancer and small cell lung cancer:
-
Non-Small Cell Lung Cancer (NSCLC): This is the most common type, accounting for about 85% of cases. It includes subtypes such as adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. NSCLC generally grows and spreads more slowly than small cell lung cancer.
-
Small Cell Lung Cancer (SCLC): This type accounts for about 15% of cases and is more aggressive. SCLC typically starts in the bronchi and spreads rapidly to other parts of the body. It is strongly associated with smoking.
What are the symptoms of lung cancer?
Lung cancer typically does not cause symptoms in its early stages. When symptoms do appear, they may include a persistent cough, chest pain, coughing up blood, shortness of breath, wheezing, hoarseness, and unexplained weight loss. If the cancer spreads to other parts of the body, it can cause bone pain, headaches, and other symptoms.
What are the risk factors for lung cancer?
The primary risk factor for lung cancer is smoking. The risk increases with the number of cigarettes smoked and the length of time a person has smoked. Other risk factors include exposure to second-hand smoke, air pollution, radon gas, asbestos, and other carcinogens. Family history and certain genetic mutations can also increase the risk.
How does tobacco use increase the risk of lung cancer?
Tobacco use is the leading cause of lung cancer, contributing to approximately 1.2 million deaths per year globally. Smoking tobacco exposes individuals to thousands of harmful chemicals, including over 69 known carcinogens, which damage lung tissue and increase the likelihood of mutations that lead to cancer. The risk of developing lung cancer is significantly higher for smokers compared to non-smokers, and the risk increases with the duration and intensity of smoking. Additionally, exposure to second-hand smoke also elevates the risk of lung cancer in non-smokers. Quitting smoking at any age can substantially reduce the risk of lung cancer and improve overall health.
For more information, visit UICC’s page on tobacco control.
How does air pollution increase the risk of lung cancer?
Nearly half of lung cancer cases in people who have never smoked are estimated to be related to air pollution, and air pollution is responsible for about 29% of all lung cancer deaths globally.
Particulate matter in polluted air can penetrate the lungs and bloodstream, causing inflammation and oxidative stress, which may damage DNA and lead to cancer. Inhalation of harmful chemicals such as benzene, formaldehyde, and polycyclic aromatic hydrocarbons also contributes to cancer risk.
Reducing exposure to air pollution, particularly in high-pollution areas, can lower the risk of developing air pollution-related cancers. Efforts to minimise pollution, such as using clean energy sources, reducing vehicle emissions, and staying indoors on high-pollution days, may also be protective.
For more information, visit UICC’s page on cancer and air pollution.
How is lung cancer diagnosed?
Lung cancer is diagnosed through a combination of imaging tests, such as chest X-rays and CT scans, and biopsy procedures where a sample of lung tissue is examined under a microscope. Additional tests, such as PET scans and MRI, may be used to determine the extent of the cancer.
What are the prevention strategies for lung cancer?
Lung cancer is a highly preventable disease, with 80-90% of cases attributed to modifiable risk factors. This means that prevention by reducing exposure to these risk factors is the most cost-efficient and highly effective strategy.
Quitting smoking at any age can significantly reduce the risk of lung cancer and improve overall health. Taxation, public health campaigns, support programmes for smokers, advertising and public smoking bans, plain packaging, and the strict regulation of other tobacco and nicotine products such as e-cigarettes, are crucial in reducing tobacco use.
Governments should act to reduce outdoor air pollution, such as using clean energy sources, reducing vehicle emissions, and creating more green spaces.
To reduce exposure to indoor air pollution, individuals can:
-
Use clean cooking fuels and technologies, such as electric stoves or improved biomass stoves.
-
Ensure proper ventilation in homes to reduce the concentration of indoor pollutants.
-
Avoid smoking indoors and implement smoke-free policies within the home.
-
Regularly clean and maintain heating and cooking appliances to prevent the buildup of harmful emissions.
Other prevention strategies include testing homes for radon, avoiding exposure to known carcinogens, and maintaining a healthy lifestyle with regular exercise and a balanced diet.
What are the treatment options for lung cancer?
Treatment options for lung cancer depend on the type and stage of the cancer. They may include surgery, radiation therapy, chemotherapy, targeted therapy, and immunotherapy. The choice of treatment is based on the specific characteristics of the cancer and the overall health of the patient.
What is the prognosis for lung cancer patients?
The prognosis for lung cancer patients varies depending on the type and stage of the cancer at diagnosis. Early-stage lung cancer has a better prognosis and may be curable with surgery. Advanced-stage lung cancer is more challenging to treat and often has a poorer prognosis. However, advances in treatment options are improving outcomes for many patients.
What actions can governments take to enhance access to early detection of lung cancer?
Governments can enhance access to early detection of lung cancer by implementing integrated approaches that combine public awareness campaigns, advanced screening technologies, and accessible healthcare services. This includes providing funding for low-dose CT screening programmes, training healthcare workers, and ensuring that screening is affordable and accessible to all, especially in low-resource settings.
Governments should also seek to address lung cancer in their national cancer plans (NCCPs). Currently, only 12% of NCCPs have lung cancer screening/early detection strategies.
How can lung cancer management overall be improved?
Improving lung cancer management involves implementing comprehensive care frameworks, such as Optimal Care Pathways, which has been developed in Australia. Optimal Care outlines best practices in cancer service delivery, from prevention and early detection to diagnosis, treatment, recovery, and end-of-life care. The pathways aim to ensure consistent, high-quality, and evidence-based care for people living with cancer.
These pathways emphasise a people-centred approach, ensuring that care is tailored to individual needs and preferences. They also stress the importance of multidisciplinary care, where expertise from various specialities is integrated to provide comprehensive support. Additionally, they highlight the need for effective care coordination, ensuring that services are streamlined across different providers, and for clear, compassionate communication between patients and their care teams.
Lung cancer-specific pathways focus on several key areas. Prevention and early detection are crucial, involving efforts to address risk factors such as smoking, air pollution, and asbestos exposure, as well as promoting screening for high-risk populations. Primary care and referral processes are also enhanced, with a focus on improving symptom awareness among healthcare providers and reducing the time to diagnosis through efficient referral systems. Once diagnosed, advanced screening tools, molecular testing, and tumour boards are used to customise treatment plans based on the cancer's stage. Finally, survivorship and end-of-life care are prioritised, ensuring access to monitoring for recurrence and palliative care when needed.
Why is there often stigma surrounding lung cancer?
The stigma surrounding lung cancer arises from the misconception that it is solely a smoker's disease and that those diagnosed with it are to blame for their condition. This stigma can lead to feelings of guilt, shame, and isolation for patients, negatively impacting their mental health and quality of life. Many people with lung cancer feel judged by others, which can exacerbate their emotional distress and make it harder for them to seek support.
Why is it important to address lung cancer stigma?
Lung cancer stigma affects patients in several ways. Emotionally, it can lead to feelings of guilt, shame, and isolation, contributing to depression and anxiety. Socially, patients may experience isolation as they feel judged or blamed by others, including friends and family. In healthcare settings, stigma can deter patients from seeking medical help early, leading to delayed diagnoses and poorer outcomes. Additionally, it can affect the level of support and empathy they receive from healthcare providers, further complicating their treatment journey.
Therefore, addressing lung cancer stigma is crucial to improving the overall well-being of patients, encouraging early detection and treatment, and ensuring that patients receive the support and empathy they need. Reducing stigma can also help to increase awareness and funding for lung cancer research and support services. By fostering a more compassionate understanding of lung cancer, we can create a more supportive environment for those affected by the disease.
Several actions can be taken to reduce lung cancer stigma. Increasing public awareness about the diverse causes of lung cancer, including genetic factors and environmental exposures, can help dispel the myth that it is solely a smoker's disease. Encouraging supportive and non-judgmental communication from healthcare providers, family, and friends can help patients feel understood and supported. Advocacy groups and campaigns can play a significant role in changing public perceptions and promoting a more compassionate understanding of lung cancer.
How does UICC support lung cancer awareness and research?
UICC leads global campaigns to raise awareness about lung cancer, its risk factors, and the importance of early detection. By collaborating with its members and partners, UICC promotes educational programs and advocacy efforts to highlight the burden of lung cancer and the need for comprehensive lung health strategies. For instance, UICC advocates for the adoption at the World Health Assembly of a resolution on promoting and prioritising an integrated lung health approach, which aims to address the growing burden of lung diseases worldwide, including lung cancer.
UICC collaborates with the World Health Organization (WHO) and the International Agency for Research on Cancer (IARC) to develop key technical resources and advocate for global commitment to the lung cancer pathway within the health community. These resources support the implementation of evidence-based policies and practices to improve lung cancer prevention, early detection, and treatment.
UICC has been leading the Lung Cancer Collaboration (LCC) Secretariat since 2023. The organisation also works closely with Permanent Missions in Geneva and governments to support lung cancer initiatives, facilitating global alignment and reinforcing national efforts.
What is the Lung Cancer Collaboration (LCC)?
The LCC is a key global initiative aimed at reducing premature mortality from lung cancer and doubling the five-year survival rate by 2030. It brings together multiple stakeholders, including civil society organisations, the private sector, policymakers, health professionals, and patient advocacy groups. The collaboration focuses on developing key actions and recommendations, publishing reports on early detection and screening, engaging with stakeholders to advance lung cancer initiatives, and working closely with WHO and IARC to develop technical resources and advocate for global commitment to lung cancer care.
What progress has been made in diagnosing and treating lung cancer, and what does the future look like?
Significant progress has been made in diagnosing and treating lung cancer. Advances in imaging technologies, such as low-dose CT scans, have improved early detection rates. New treatments, including targeted therapies and immunotherapies, have increased survival rates and improved the quality of life for many patients. The future of lung cancer care looks promising with ongoing research and development of new diagnostic tools and treatments, aiming to further improve outcomes and potentially find a cure.
Latest UICC news and blog articles on lung cancer
Screening for change in lung cancer diagnosis: turning the tide with technology and trust

A hidden epidemic: the rise of lung cancer among women and the need for equity

Why clean air matters for cancer care and people living with cancer

References
-
Ferlay J, Laversanne M, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2024). Global Cancer Observatory: Cancer Tomorrow. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/tomorrow, accessed 1 March 2024.
-
https://www.cancer.org/cancer/types/lung-cancer/causes-risks-prevention/risk-factors.html
-
U.S. Dept of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. U.S. Dept of Health and Human Services; 2014.
-
GBD 2019 Tobacco Collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: a systematic analysis from the Global Burden of Disease Study 2019
-
Leiter, A., Veluswamy, R.R. & Wisnivesky, J.P. The global burden of lung cancer: current status and future trends. Nat Rev Clin Oncol 20, 624–639 (2023). https://doi.org/10.1038/s41571-023-00798-3
-
Rentschler J, Leonova N. Global air pollution exposure and poverty. Nat Commun. 2023 Jul 22;14(1):4432. doi: 10.1038/s41467-023-39797-4. PMID: 37481598; PMCID: PMC10363163.
-
https://www.lung.org/research/state-of-lung-cancer/key-findings
-
https://www.cancerresearchuk.org/about-cancer/lung-cancer/survival
-
Field JK, Vulkan D, Davies MPA, Baldwin DR, Brain KE, Devaraj A, Eisen T, Gosney J, Green BA, Holemans JA, Kavanagh T, Kerr KM, Ledson M, Lifford KJ, McRonald FE, Nair A, Page RD, Parmar MKB, Rassl DM, Rintoul RC, Screaton NJ, Wald NJ, Weller D, Whynes DK, Williamson PR, Yadegarfar G, Gabe R, Duffy SW. Lung cancer mortality reduction by LDCT screening: UKLS randomised trial results and international meta-analysis. Lancet Reg Health Eur. 2021 Sep 11;10:100179. doi: 10.1016/j.lanepe.2021.100179. PMID: 34806061; PMCID: PMC8589726.
-
Poon C, Wilsdon T, Sarwar I, Roediger A and Yuan M (2023) Why is the screening rate in lung cancer still low? A seven-country analysis of the factors affecting adoption. Front. Public Health 11:1264342. doi: 10.3389/fpubh.2023.1264342.
-
https://iris.who.int/bitstream/handle/10665/254500/9789241511940-eng.pdf?sequence=1
-
https://www.cancer.org.au/assets/pdf/lung-cancer-quick-reference-guide
Last update
Wednesday 14 May 2025